
 Request an Appointment
Request an Appointment Request Online Consultation
Request Online Consultation Enquiry form
Enquiry form







Chordomas & Craniopharyngioma
Chordomas
Usually, these tumors grow slowly at the base of the skull and the lower part of the spine. They are mostly seen among individuals at the age group of 50-60. Even though they are non-cancerous, they may cause excess pressure on the nearby neural tissues. They derive from the remnants of the embryonic notochord. They are incessant and may recur even after a course of treatment. Main treatment option for chordomas is the surgery. With the surgery, the tumor can be removed partially, or completely. Chordomas are very rare, which contribute only 0.2% of all primary brain tumors hh hfd b vfhndc.
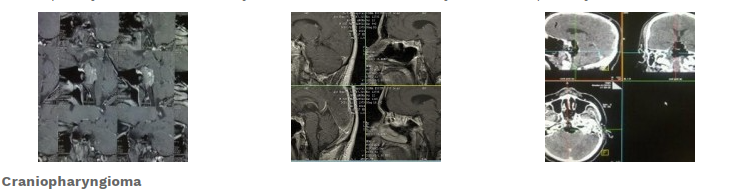
Craniopharyngioma
They derive from the embryogenic remnants in the core of Pituitary Gland. These benign tumors may even attack the surrounding structures also. They will have both cystic as well as solid components. It is difficult to discover craniopharyngiomas in an individual unless it press or invade the vital structures that surround the hypothalamus or the optic nerve region. The most common symptoms seen in children affected by Craniopharyngioma are:
- Headache
- Lack of growth
- Precocious puberty
- Vomiting etc.
Visual field defect is the most common symptom seen among adults with Craniopharyngioma. Overall incidents of Craniopharyngioma are calculated as 0.18 per 100,000 people per years. The condition may not vary according to gender or race. 4.1% of tumors that affect the children are Craniopharyngioma.
Diagnosis:
The best method used for diagnosing Craniopharyngiomas is an MRI with contrast.
Treatment:
The most preferred treatment is microsurgical excision and a Transcranial route through craniotomy. Procedures such as Expanded Endonasal Approach and Endoscopic removal of tumors are also chosen in certain cases. The surgery will have 86-99% of success rates. The condition may recur even after the complete removal. Radiation and or Intra tumoral Bleomycin are used for recurrence or residual tumor.
Our Doctors

Dr Manish Vaish - Director
Director, Delhi

Dr. Yashpal Bundela MS Mch
Associate Director-Neurosurgery

Dr.Girish Rajpal MS Mch FINR
Neurointerventional Surgeon

Dr Hrishikesh Chakrabartty
Senior Consultant Neurosurgeon

Dr.Praveen Kumar MS Mch
Senior Consultant Neurosurgeon

Dr Rohit Pandey
Neurosurgeon

Dr Dipanshu Narula
Neurosurgeon

Dr. Manish Marda MD DM
Head of Neuroanesthesia, pain management and critical care

Dr. Shiwani Jain MD FNB
Senior consultant Neuroanesthesia, pain and critical care
Videos



Testimonial

Patient Testimonial - Santosh Kumari

Brain Tumor Treatment Patient Experience In Ghaziabad | Brain Tumor Surgery | Neurosurgeon In India

Neck Pain Treatment In Delhi | Spinal Cord Surgeon In Ghaziabad | Neurosurgeon In India

Spinal Injury Treatment In Ghaziabad | Spinal Cord Surgeon In Delhi, India

Spine Surgery For Back Pain In Ghaziabad | Lumbar Spinal Stenosis Treatment In Delhi, India

Spinal Cord Surgery In Ghaziabad | Slip Disc Treatment In Delhi, India

Successfull Skull Base Tumor Surgery In Noida | Brain Tumour Treatment In Uttar Pradesh, India

Back Pain Treatment In Uttar Pradesh - Patient Testimonial

Brain Tumor Patient Testimonial| Brain Tumor Surgery In Uttar Pradesh| Neurosurgeon| Dr Manish Vaish
